
Type 1 Diabetes
The Treatment for Type 1 Diabetes

The
treatment must be lifelong insulin replacement. Insulin treatment may
be difficult to use. Insulin must be injected, and the dose must be
closely adjusted to avoid high or low blood sugars in the presence of
varying levels of physical activity, food intake and the physical state
of the person taking the insulin. Since Banting’s and Best’s discovery
of insulin, there have been major changes in the production and
manufacture of insulin to improve the consistency and quality of
insulin products. We have now moved away from animal derived insulin
and most insulin currently sold is genetically engineered from
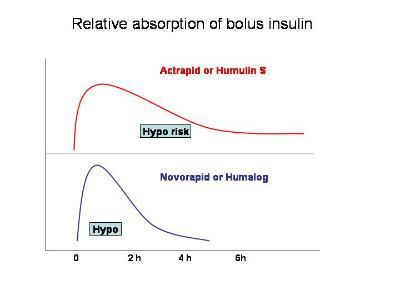
bacteria. The insulin that is then produced is either stabilised
without retardant, soluble insulin (Actrapid or Humulin S) or is
crystallised or retarded with other agents (Ultratard, Humulin I and
Insulatard). A small amount of animal derived insulin is still used by
patients who have been stabilised on it, and in whom there is no
clinical indication to switch to human insulin.
The Process of Insulin Administration
Insulin
is given by injection, and this has been improved with development of
the pen syringes. These devices still require an injection, but are
more convenient to carry and speed up insulin administration. They
enable multiple insulin injections throughout the day, and can be
filled with a variety of types of insulin mixes to match the individual
requirements. The new class of analogue insulin represents an exciting
development in insulin therapy. These are genetically engineered
insulins, in which the amino acids are altered to different sites to
alter the physical characteristics and actions of insulin. Currently
two products, Lispro insulin (Humalog)and Insulin Aspart (Novorapid) are available.
These
insulins are more rapidly acting than conventional human insulin, and
enable the person with diabetes to have less fluctuation in blood
glucose after meals, to have fewer episodes of hypoglycaemia and
reduced weight gain with improved overall glycaemic control when
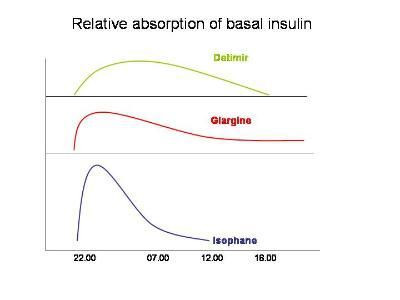
compared with soluble insulin. A further analogue insulin, Insulin Glargine
(Lantus), has been recently released. This insulin has a “flatter”
action profile, with a markedly prolonged length of action. This
profile offers the possibility of improved basal action, with less
nocturnal hypoglycaemia and lower fasting blood glucose concentrations.
The combination of this analogue with one of the shorter acting
analogues looks very promising in the search for an insulin regime that
supports normal post-meal excursions of glucose concentrations without
fasting hypoglycaemia. Recently, a further new insulin, Detimir, has
been release which seems very predictable in it's action, with a
typical duration of about 14-16 hours
However, even with these improvements, insulin treatment will continue to be difficult until we have automatic and self-governing insulin administration devices, or grafts of genetically manipulated insulin secreting cells.
However, even with these improvements, insulin treatment will continue to be difficult until we have automatic and self-governing insulin administration devices, or grafts of genetically manipulated insulin secreting cells.
Contact us
In order to visit us
Runsweet.com
Royal Berkshire Centre For Diabetes and Endocrinology
Reading
RG1 5BS
News
Find us on the Internet
Now you can go online to find out about our services.